
A doctor ventures into the field "we still lag far behind abroad", twice selects a case "no one has done" in Vietnam
Instead of choosing facial aesthetic surgery, which is a "money‑making" field, Associate Professor Chơn entered a more challenging field because he wants Vietnamese patients to be treated with technology and techniques like those in advanced countries.
When mentioning Associate Professor Dr. Hồ Nguyễn Thanh Chơn, Head of the Department of Maxillofacial Surgery – Oral and Maxillofacial Surgery at the University Hospital of Ho Chi Minh City, people often recall a teacher with both heart and vision in the field of Maxillofacial Surgery. He constantly explores to apply advanced methods and techniques from around the world and made a landmark first for patients in Vietnam.
1. Pioneering the first surgeries in Vietnam
Ngọc Minh: I still hear doctors in the medical field say that maxillofacial surgery is a hot profession, making a lot of money?
Associate Professor Hồ Nguyễn Thanh Chơn: In maxillofacial surgery there is aesthetic facial contouring, which includes orthognathic surgery and facial contour creation, indeed a hot field in Vietnam. If a doctor performs it regularly and does it well, the income is very high.
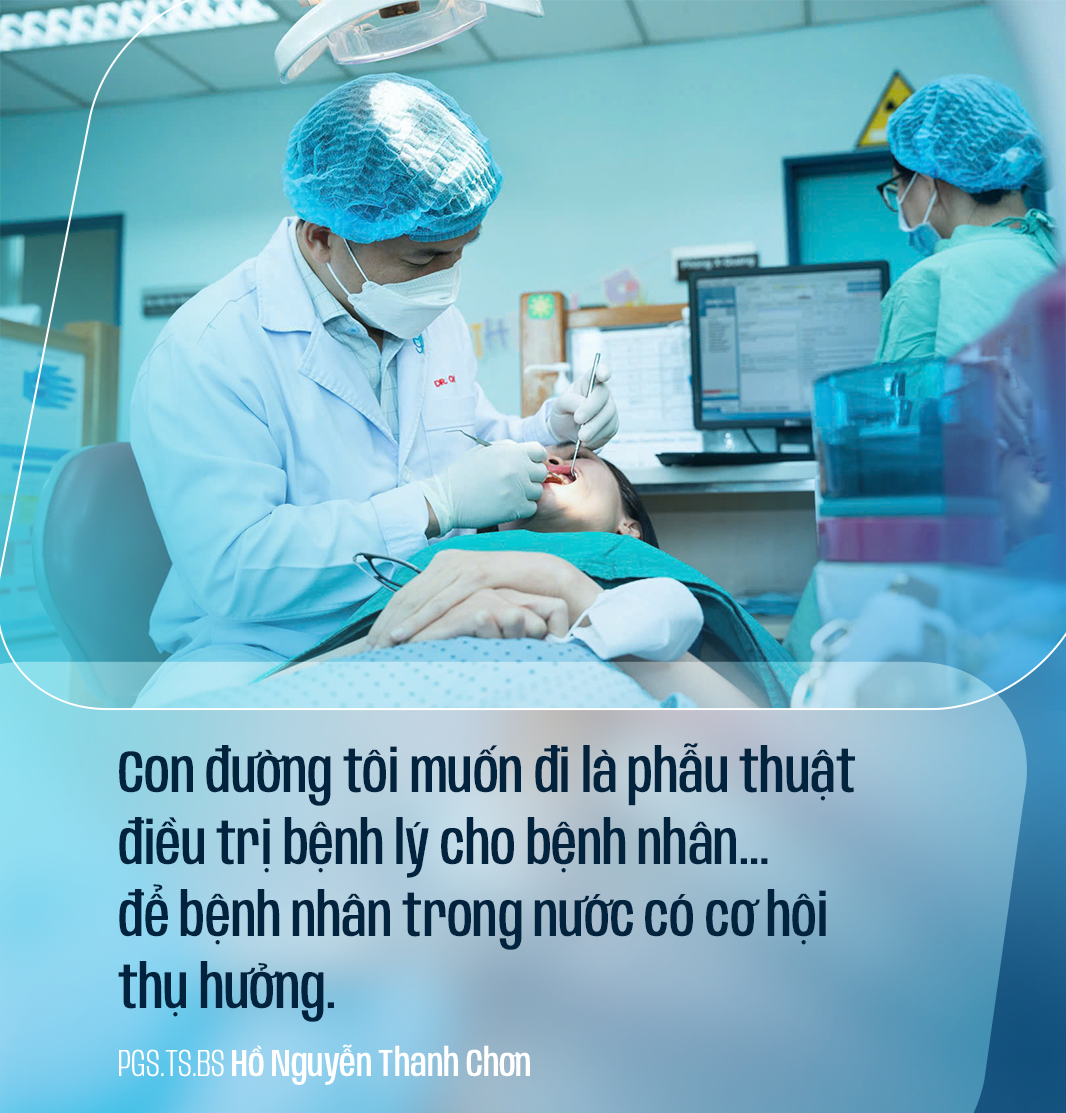
However, I have also performed many of them but have not focused too much on those surgeries. The path I want to pursue is therapeutic surgery for patients. This is also an area in Vietnam that needs to be improved further to keep pace with global advancements, so that domestic patients have the opportunity to benefit.
Ngoc Minh: Why do you still plunge into a path that you know is difficult?
Associate Professor Ho Nguyen Thanh Chon: Facial surgeons in Vietnam are now very skilled and do a great job. However, regarding pathology, I feel the need to update and learn from abroad a lot; we are still far behind them, so patients suffer disadvantages. Therefore, I will focus the remaining time on pathological surgery.
Ngoc Minh: I understand that you are one of the few who performed the first bilateral artificial temporomandibular joint replacement cases in Vietnam?
Associate Professor Ho Nguyen Thanh Chon: That's correct, I performed it together with my colleague. I still remember it was a case where the patient had an accident, then developed a stiff temporomandibular joint and could not open his mouth. For many years the patient could only drink and eat pureed food.
Previously, the patient had undergone surgery several times, but after a while, the joint adhered again, causing the patient to be "afraid" of surgery, and the quality of life also declined because the mouth could not open.
I have always been concerned, wondering if there is a way to help the patient. At that time, my colleagues and I went abroad to study the technique of artificial temporomandibular joint replacement and thought we could do it for that patient.
However, learning is one thing, but having never performed it, I was also anxious. The worry here is not that I cannot do it, but that after surgery the results may not meet expectations. Since artificial TMJ prostheses are very expensive, a failure would be very costly for the patient.
We strived to perfect the technique to perform a bilateral temporomandibular joint replacement. This TMJ replacement surgery became the first case of bilateral artificial joint replacement in Vietnam.
After the surgery, the patient was able to open his mouth immediately. To date, the patient has not experienced re-adhesion, and his quality of life has improved.
Ngoc Minh: He is also the first in Vietnam to perform endoscopic combined surgery of a fractured condylar neck and lower jaw via endoscopy. This work has become a "model paper" for specialists to refer to regarding this surgery.
Associate Professor Ho Nguyen Thanh Chon: For me, the teachers in the field of maxillofacial surgery are very skilled, and I have a lot to learn. I just try to be a pioneer, doing things that the teachers and colleagues have not had time to research yet.
For that reason, my PhD thesis was on combined surgery for fractured mandibular condyle and lower jaw via endoscopy. I began researching and performing this surgery in 2012, and I hope that what I do will bring real benefits to patients.
Previously, surgery for fractured mandibular condyle and lower jaw required an external incision, which easily left unsightly scars and could cause facial nerve palsy (mouth distortion). If I can perform endoscopic surgery through the intraoral route, the patient will not have unsightly scars or mouth distortion.
In 2016, I successfully defended my PhD thesis. This research marked the first time Vietnam performed endoscopic surgery for fractured mandibular condyle and lower jaw.
Later, I published an international journal article on this work, which was highly praised by colleagues.
Recently, I compiled it into a reference book so that specialists can study and refer to it.
I always believe that whatever I can achieve, I will strive to pioneer and help patients. The pioneers may face difficulties and barriers, but persisting will eventually reach the goal. If you don't act, you'll never achieve anything.
2. Aspiration to become a surgeon like my mother
Ngoc Minh: In the 1990s, facial jaw surgery was still quite new; why did you decide to pursue it?
Associate Professor Hồ Nguyễn Thanh Chơn: It started from my personal passion, thanks to my mother being a general external surgeon. Since I was 3 years old I followed my mother into the operating room. Seeing my mother as the "commander-in-chief" of the surgery, I always dreamed that one day I would be like her. In my essays I always wrote about my dream of becoming a doctor.
But the times changed in the 1990s, I saw many of my fellow graduates from medical school without jobs. Many had to work outside their profession, some had to retake exams to study a different field. I was very uncertain whether I should pursue medical school.
Finally I decided to still take the entrance exam for medical school but to study Dentistry. I thought this field would allow me to work independently after graduation. If I couldn't get a job at hospitals, I could open a dental clinic. I shared this intention with my mother. My mother was not happy because she wanted me to become a surgeon.
I was admitted in my first year to the University of Medicine and Pharmacy in Ho Chi Minh City and studied Dentistry. The more I studied, the more I was attracted to the specialty of maxillofacial surgery. In 1999, after graduating as a dentist, I took the maxillofacial surgery residency exam. That year, there were three residency slots for maxillofacial surgery but only I was accepted.
In that residency program, I had to study and do clinical rotations at the hospital all by myself. Suddenly I became a "rare" student. I remember I was the fourth person (from 1975–1999) to be admitted to the maxillofacial surgery residency at the University of Medicine and Pharmacy in Ho Chi Minh City.
Ngọc Minh: PGS, do you still remember the first case where you acted as the chief surgeon?
PGS Hồ Nguyễn Thanh Chơn: Of course, I have. When I was still a resident, the teachers were very strict. I spent a long time assisting surgeries at night, but I still hadn't performed any surgeries.
I remember sometime in my second year of residency, after having assisted many surgeries, a senior surgeon told me: "Chơn, operate this case, I'll assist". Given the opportunity, I worked hard to do my best. I succeeded in that operation and received high praise from the senior surgeons who guided me.
Ngọc Minh: I've heard that maxillofacial surgery is less demanding compared to other surgical specialties and has fewer complications; is this true?
PGS Hồ Nguyễn Thanh Chơn: Maxillofacial surgery does not have a high mortality rate on the operating table like brain or heart surgery. However, sudden situations can occur. I have witnessed a patient suffer a facial region injury from an accident; the doctor did not have time to intervene and the patient died. Because the patient bled profusely, the doctor couldn't perform a tracheostomy in time, and blood flooded the airway.
Having seen that case since my residency, I still remind my students: Bone injury from a facial trauma may not kill the patient, but uncontrolled airway bleeding without timely emergency care will cause death.
Ngọc Minh: I understand that PGS often participates in humanitarian surgeries for children with cleft lip, palate, and mandibular deformities?
Associate Professor Ho Nguyen Thanh Chon: I have been participating in this program since I was a resident. And I see that almost every maxillofacial surgeon also participates in this meaningful surgery program. This is something that should be done for patients.
I also have a bond with the program for almost 25 years. Each charitable surgery is an unforgettable memory.
Currently, the incidence of cleft lip and palate in Vietnam is about 1/500 of the newborn population. A case of cleft lip and palate that requires surgical treatment to return relatively to normal will need to go through more than 10 treatment stages with many surgeries, consuming a great amount of time and effort for both patients and doctors. Patients will receive continuous treatment to achieve the most balanced facial appearance upon adulthood.
3. The doctor can sometimes be very “tough” but very demanding
Ngoc Minh: I heard rumors that PGS is a simple and approachable person in real life. Working with PGS must be easy, right?
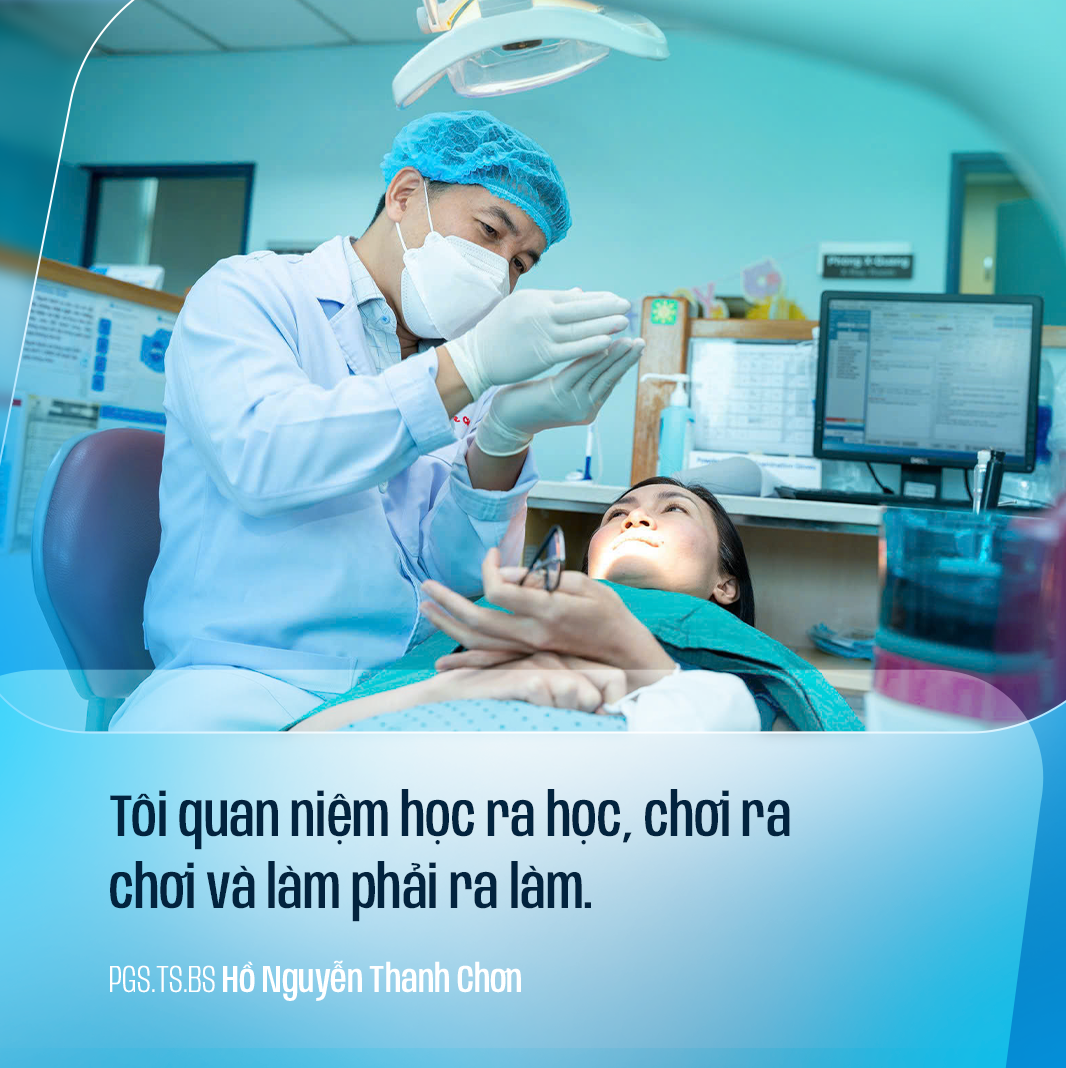
PGS Ho Nguyen Thanh Chon: I believe in learning when it's time to learn, playing when it's time to play, and working when it's time to work. In my job I am a perfectionist, so sometimes I feel I am strict with students and staff. I always want everyone, when treating and caring for patients, to treat the patient as a family member. Therefore, the treatment outcomes for patients must be as perfect as possible; I always want my students to do it correctly, exactly as I would.
It cannot be denied that there are times when I also act like a "bear" (stern) with my students. The work needs to be precise, so one must always maintain an attitude of respecting patients and set an example for everyone.I have also heard somewhere that when working with me, people feel pressure. But I think that pressure is necessary for the students to improve.
However, I am also a very open-minded person. When a student says something correct, I always acknowledge it and follow it. I am not authoritarian or conservative, so the students are approachable. I greatly appreciate those who dare to point out things that are not yet truly good so that we can improve even more for the patients. Let me give a simple example: I am the lead surgeon, with only two eyes during the operation, focusing all my attention on the main lesions, I might miss other things; thanks to the eyes of the students or members of the surgical team, they can spot other issues, and if they sense that I am approachable, they will inform me immediately.